Quality Metrics¶
Guide to computing treatment plan quality metrics in dosemetrics.
Try Quality Metrics in Live Demo
Overview¶
Plan quality metrics quantify how well a radiotherapy treatment plan delivers the intended dose to the target while sparing surrounding healthy tissue. dosemetrics implements three families of such metrics:
| Family | What it measures | Key functions |
|---|---|---|
| Conformity | How well the high-dose region matches the target shape | compute_conformity_index, compute_paddick_conformity_index, compute_rtog_conformity_index, compute_conformity_number, compute_coverage, compute_spillage, compute_prescription_mae |
| Homogeneity | How uniform the dose is within the target | compute_homogeneity_index, compute_gradient_index, compute_dose_homogeneity, compute_uniformity_index |
| DVH comparison | Aggregate differences between two dose distributions | compute_dvh_score, compute_dvh_auc, compute_normalized_mae, compute_variance_of_laplacian |
All functions follow the same calling convention: they accept a Dose object, one or two Structure objects, and any numeric parameters, and return a plain float.
Conformity Indices¶
Conformity indices measure the spatial relationship between the prescription isodose and the target volume. A perfect plan has a prescription isodose that exactly coincides with the target: no tissue outside the target is irradiated to prescription dose, and no part of the target is missed.
The three key volumes involved are:
- V_target — total target volume (all voxels in the target structure)
- V_rx — prescription isodose volume (all voxels with dose ≥ prescription)
- V_target_rx — overlap: voxels that are both inside the target and receive ≥ prescription dose
ICRU Conformity Index (compute_conformity_index)¶
$$\text{CI} = \frac{V_{\text{target_rx}}}{V_{\text{rx}}}$$
Introduced in ICRU Report 62 (1999). Measures what fraction of the prescription isodose volume actually covers the target.
- Ideal value: 1.0 (all irradiated tissue is inside the target)
- < 1.0: dose spills outside the target
- = 0: the prescription isodose does not overlap the target at all
van't Riet and the Conformity Number
This CI formula is closely related to the Conformation Number (CN) introduced by van't Riet et al. (1997). The CN additionally penalises undercoverage:
$$\text{CN} = \frac{V_{\text{target_rx}}}{V_{\text{target}}} \times \frac{V_{\text{target_rx}}}{V_{\text{rx}}}$$
CN = 1.0 only when every target voxel is covered and no dose spills outside. Use compute_conformity_number for this.
Reference: van't Riet A, et al. Int J Radiat Oncol Biol Phys. 1997;37(3):731-736.
from dosemetrics.metrics.conformity import compute_conformity_index, compute_conformity_number
ci = compute_conformity_index(dose, ptv, prescription_dose=60.0)
cn = compute_conformity_number(dose, ptv, prescription_dose=60.0)
print(f"ICRU CI: {ci:.3f}") # Ideal: 1.0
print(f"CN: {cn:.3f}") # Ideal: 1.0
RTOG Conformity Index (compute_rtog_conformity_index)¶
$$\text{RTOG\ CI} = \frac{V_{\text{rx}}}{V_{\text{target}}}$$
Defined in the RTOG 90-05 stereotactic radiosurgery protocol (Shaw et al. 1993). Asks: "how many times larger is the prescription isodose than the target?"
- Ideal value: 1.0
- > 1.0: prescription isodose is larger than the target (spillage)
- < 1.0: prescription isodose is smaller than the target (undercoverage)
RTOG acceptance criteria for radiosurgery:
| RTOG CI range | Grade |
|---|---|
| 1.0 – 2.0 | Acceptable |
| < 1.0 or 2.0 – 2.5 | Minor deviation |
| > 2.5 | Major deviation |
RTOG CI vs ICRU CI
These two CIs are different metrics. The ICRU CI (V_target_rx / V_rx) measures the purity of the isodose — how much of the irradiated region is target. The RTOG CI (V_rx / V_target) measures the size ratio between the isodose and the target. With significant dose spillage, RTOG CI > 1 while ICRU CI < 1.
from dosemetrics.metrics.conformity import compute_rtog_conformity_index
rtog_ci = compute_rtog_conformity_index(dose, ptv, prescription_dose=60.0)
if 0.9 <= rtog_ci <= 1.1:
print("Excellent conformity")
elif 1.0 <= rtog_ci <= 2.0:
print("Acceptable (RTOG 90-05)")
else:
print("Deviation from protocol")
Reference: Shaw E, et al. Int J Radiat Oncol Biol Phys. 1993;27(5):1231-9.
Paddick Conformity Index (compute_paddick_conformity_index)¶
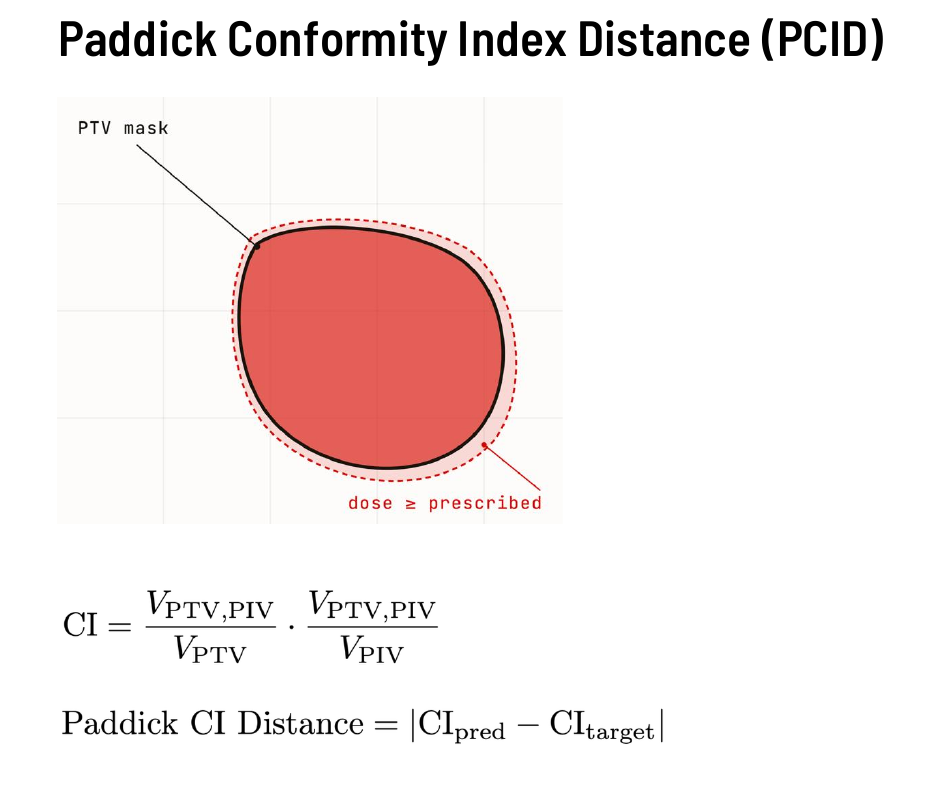 Paddick Conformity Index Distance (PCID) — the prescription isodose volume (dashed red) overlaps the PTV mask (solid black). CI is the product of target coverage and target conformity; PCID is the absolute difference in CI between two plans. (Joseph Weibel, MSc Thesis Defense, University of Bern)
Paddick Conformity Index Distance (PCID) — the prescription isodose volume (dashed red) overlaps the PTV mask (solid black). CI is the product of target coverage and target conformity; PCID is the absolute difference in CI between two plans. (Joseph Weibel, MSc Thesis Defense, University of Bern)
$$\text{CI}{\text{Paddick}} = \frac{V$$}}^2}{V_{\text{target}} \times V_{\text{rx}}
Proposed by Paddick (2000) as a single metric that simultaneously penalises both undercoverage and dose spillage. It is the product of target coverage and target conformity:
$$\text{CI}{\text{Paddick}} = \underbrace{\frac{V}}}{V_{\text{target}}}{\text{coverage}} \times \underbrace{\frac{V$$}}}{V_{\text{rx}}}}_{\text{conformity}
- Ideal value: 1.0 (only when coverage = 1 and conformity = 1)
- < 1.0: either part of the target is missed, or dose spills into normal tissue, or both
The Paddick CI is the most widely used single conformity metric for stereotactic radiosurgery (SRS) and SBRT, where tight conformity around small targets is critical.
Paddick CI vs van't Riet CN
The Paddick CI and the van't Riet CN share the same formula. The CN was independently defined by van't Riet (1997); Paddick arrived at the same expression from a different motivation in 2000. dosemetrics exposes both names (compute_paddick_conformity_index and compute_conformity_number) pointing to the same computation.
from dosemetrics.metrics.conformity import compute_paddick_conformity_index
ci_paddick = compute_paddick_conformity_index(dose, gtv, prescription_dose=18.0)
print(f"Paddick CI: {ci_paddick:.3f}") # 1.0 = perfect
Reference: Paddick I. J Neurosurg. 2000;93(Suppl 3):219-222.
Coverage (compute_coverage)¶
$$\text{Coverage} = \frac{V_{\text{target_rx}}}{V_{\text{target}}}$$
The fraction of the target volume that receives at least the prescription dose. Identical to the first term of the Paddick/van't Riet CI. Sometimes called D95 ≥ Rx coverage when evaluated at the 95% volume threshold.
from dosemetrics.metrics.conformity import compute_coverage
cov = compute_coverage(dose, ptv, prescription_dose=60.0)
print(f"Target coverage: {cov * 100:.1f}%")
Spillage (compute_spillage)¶
$$\text{Spillage} = \frac{V_{\text{rx}} - V_{\text{target_rx}}}{V_{\text{rx}}}$$
The fraction of the prescription isodose volume that lies outside the target. Complementary to compute_conformity_index (they sum to 1).
from dosemetrics.metrics.conformity import compute_spillage
spillage = compute_spillage(dose, ptv, prescription_dose=60.0)
print(f"Dose spillage: {spillage * 100:.1f}%")
Prescription MAE (compute_prescription_mae)¶
$$\text{Prescription MAE} = \frac{1}{|V_{\text{target}}|} \sum_{v \in V_{\text{target}}} \lvert d_v - d_{\text{rx}} \rvert$$
The mean absolute deviation of the dose inside the target from the prescription dose. Unlike conformity indices, this metric is sensitive to both underdosing and overdosing within the target.
- 0 Gy: every voxel in the target received exactly the prescription dose (ideal)
- > 0 Gy: average deviation from prescription; useful for reporting alongside CI to characterise the degree of miss
from dosemetrics.metrics.conformity import compute_prescription_mae
mae = compute_prescription_mae(dose, ptv, prescription_dose=60.0)
print(f"Prescription MAE: {mae:.2f} Gy ({mae / 60.0 * 100:.1f}% of prescription)")
Reference: Adapted from PTVPrescriptionMAE in the GDP-HMM AAPM Challenge evaluation.
Choosing a Conformity Metric¶
| Scenario | Recommended metric |
|---|---|
| Standard IMRT/VMAT protocol reporting | ICRU CI + Coverage |
| SRS/SBRT plan evaluation | Paddick CI |
| RTOG protocol compliance | RTOG CI |
| Quantifying overdosing magnitude | Prescription MAE |
| Full picture: coverage + spillage | van't Riet CN (= Paddick CI) |
Homogeneity Indices¶
Homogeneity indices measure the uniformity of dose within the target volume. A perfectly homogeneous plan delivers the same dose to every voxel inside the target.
ICRU Homogeneity Index (compute_homogeneity_index)¶
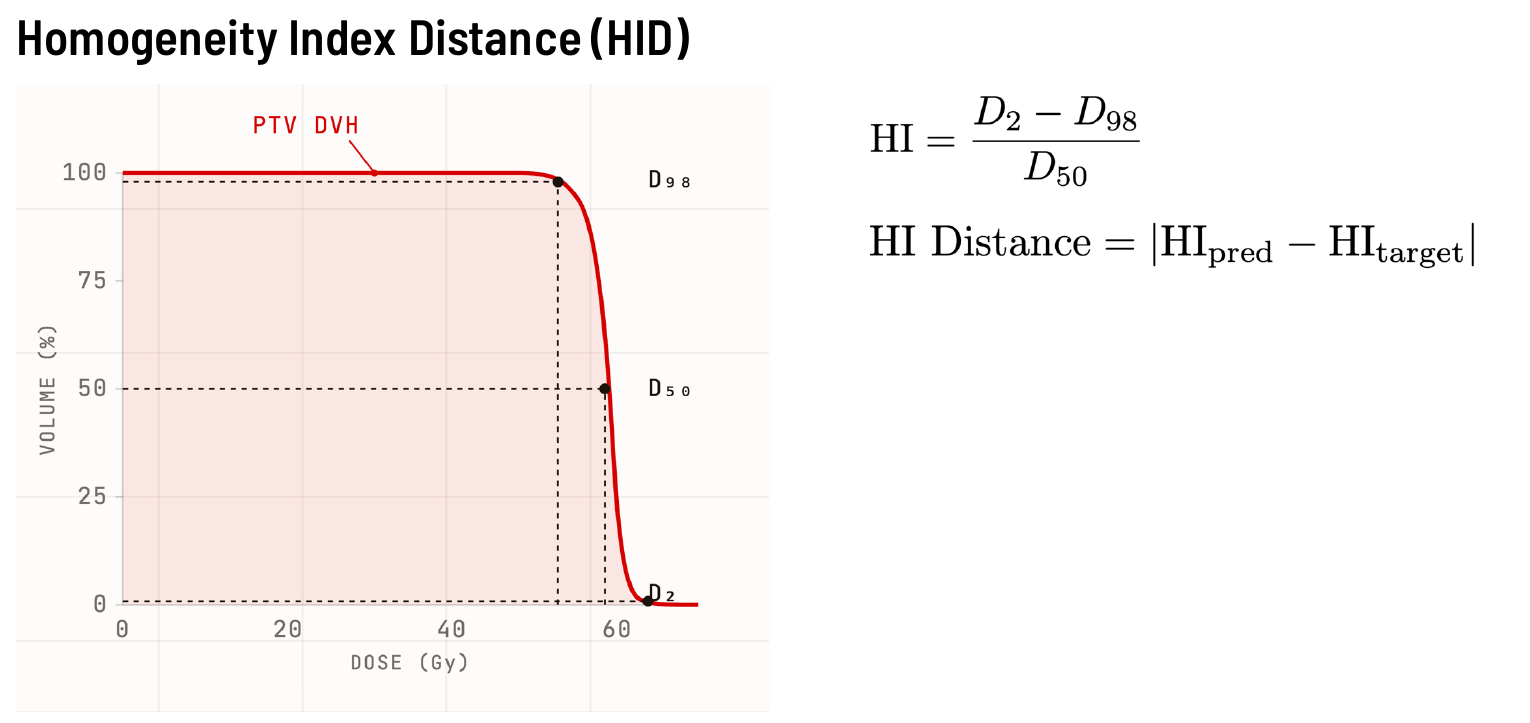 Homogeneity Index Distance (HID) — D₂ (near-maximum), D₅₀ (median), and D₉₈ (near-minimum) are read from the PTV DVH. The shaded area illustrates the dose band between D₂ and D₉₈. HID is the absolute difference in HI between two plans. (Joseph Weibel, MSc Thesis Defense, University of Bern)
Homogeneity Index Distance (HID) — D₂ (near-maximum), D₅₀ (median), and D₉₈ (near-minimum) are read from the PTV DVH. The shaded area illustrates the dose band between D₂ and D₉₈. HID is the absolute difference in HI between two plans. (Joseph Weibel, MSc Thesis Defense, University of Bern)
$$\text{HI} = \frac{D_2 - D_{98}}{D_{50}}$$
Where $D_X$ is the dose received by at least $X\%$ of the target volume ($D_2$ ≈ near-maximum, $D_{98}$ ≈ near-minimum). Defined in ICRU Report 83 (2010).
- Ideal value: 0.0 (perfectly uniform dose)
- Typical acceptable range: 0.05 – 0.20
- Higher values: greater dose non-uniformity (hot/cold spots)
from dosemetrics.metrics.homogeneity import compute_homogeneity_index
hi = compute_homogeneity_index(dose, ptv)
print(f"HI: {hi:.3f}")
if hi < 0.10:
print("Excellent homogeneity")
elif hi < 0.20:
print("Acceptable homogeneity (ICRU 83)")
else:
print("Consider plan revision")
Reference: ICRU Report 83. J ICRU. 2010;10(1).
Gradient Index — Paddick & Lippitz (compute_gradient_index)¶
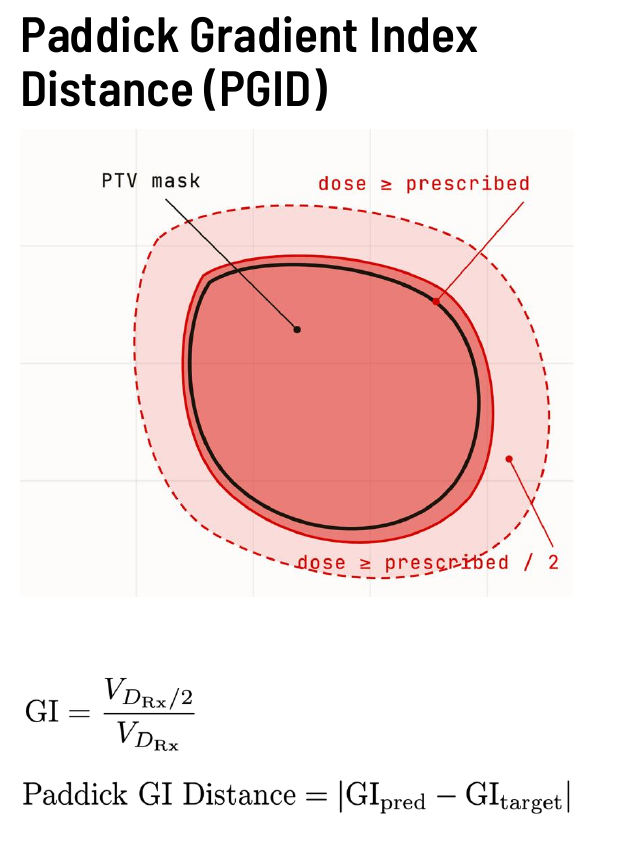 Paddick Gradient Index Distance (PGID) — the ratio of the half-prescription isodose volume (outer dashed region) to the full-prescription isodose volume (inner dashed region) measures how steeply dose falls off outside the PTV. PGID is the absolute difference in GI between two plans. (Joseph Weibel, MSc Thesis Defense, University of Bern)
Paddick Gradient Index Distance (PGID) — the ratio of the half-prescription isodose volume (outer dashed region) to the full-prescription isodose volume (inner dashed region) measures how steeply dose falls off outside the PTV. PGID is the absolute difference in GI between two plans. (Joseph Weibel, MSc Thesis Defense, University of Bern)
$$\text{GI} = \frac{V_{50\%}}{V_{100\%}}$$
Where $V_{100\%}$ is the volume receiving ≥ prescription dose and $V_{50\%}$ is the volume receiving ≥ half the prescription dose. Proposed by Paddick and Lippitz (2006) to quantify how steeply dose falls off outside the target.
- Lower GI: steeper dose falloff → better normal tissue sparing
- Higher GI: more gradual falloff → larger low-dose bath
GI is particularly useful for SRS, where steep dose gradients protect the brain around a small target.
from dosemetrics.metrics.homogeneity import compute_gradient_index
gi = compute_gradient_index(dose, ptv, prescription_dose=18.0)
print(f"Gradient Index: {gi:.2f}") # Typical range 2–5 for SRS
Reference: Paddick I, Lippitz B. J Neurosurg. 2006;105(Suppl):194-201.
Coefficient of Variation (compute_dose_homogeneity)¶
$$\text{CV} = \frac{\sigma_d}{\bar{d}}$$
Standard deviation of dose in the target divided by the mean dose. A classical statistics-based homogeneity measure independent of prescription dose.
from dosemetrics.metrics.homogeneity import compute_dose_homogeneity
cv = compute_dose_homogeneity(dose, ptv)
print(f"Dose CV: {cv:.3f}")
Uniformity Index (compute_uniformity_index)¶
$$\text{UI} = 1 - \frac{D_{\max} - D_{\min}}{D_{\text{ref}}}$$
Where $D_{\text{ref}}$ is the median dose. Values closer to 1.0 indicate more uniform dose distributions.
from dosemetrics.metrics.homogeneity import compute_uniformity_index
ui = compute_uniformity_index(dose, ptv)
print(f"Uniformity Index: {ui:.3f}") # 1.0 = perfectly uniform
DVH Comparison Metrics¶
These metrics compare two dose distributions by summarising differences in their dose-volume histograms, making them useful for plan comparison and automated prediction evaluation.
DVH Score (compute_dvh_score)¶
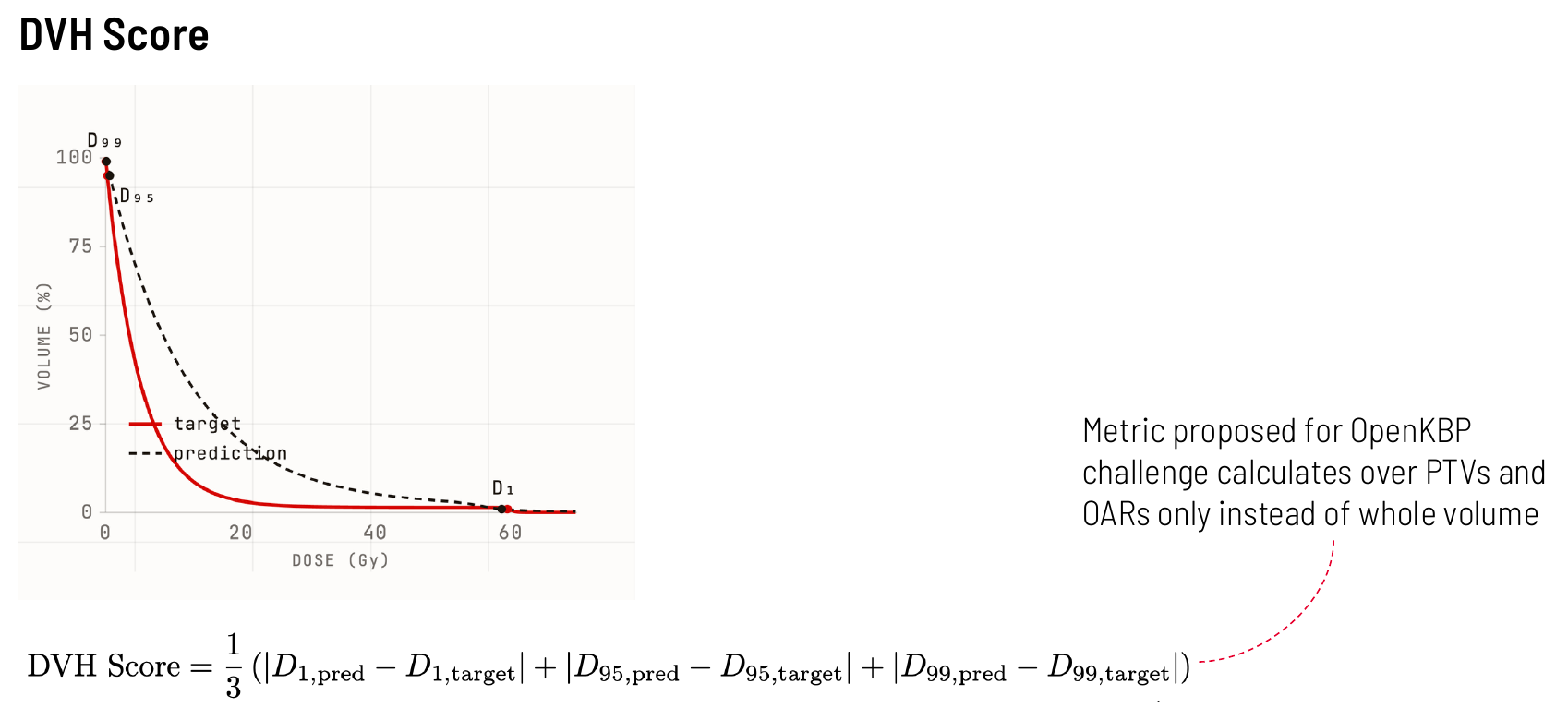 DVH Score — D₁, D₉₅, and D₉₉ are read off for both the target (solid red) and predicted (dashed) DVH curves. The score is the average of the three absolute differences. (Joseph Weibel, MSc Thesis Defense, University of Bern)
DVH Score — D₁, D₉₅, and D₉₉ are read off for both the target (solid red) and predicted (dashed) DVH curves. The score is the average of the three absolute differences. (Joseph Weibel, MSc Thesis Defense, University of Bern)
$$\text{DVH Score} = \frac{1}{3}\left(\lvert D_1^{\text{ref}} - D_1^{\text{eval}} \rvert + \lvert D_{95}^{\text{ref}} - D_{95}^{\text{eval}} \rvert + \lvert D_{99}^{\text{ref}} - D_{99}^{\text{eval}} \rvert\right)$$
The average absolute difference in three clinically important DVH dose points:
| Point | Meaning |
|---|---|
| $D_1$ | Near-maximum dose (1% of volume receives at least this) |
| $D_{95}$ | Coverage dose (95% of volume receives at least this) |
| $D_{99}$ | Near-minimum dose (99% of volume receives at least this) |
- 0 Gy: perfect agreement at all three points
- Higher: larger clinical discrepancy between the two distributions
DVH Score was used in the GDP-HMM AAPM dose-prediction challenge to assess how well AI-predicted plans reproduced the DVH of clinical plans.
from dosemetrics.metrics.dvh import compute_dvh_score
score = compute_dvh_score(reference_dose, predicted_dose, ptv)
print(f"DVH Score (PTV): {score:.2f} Gy")
Reference: Adapted from GDP-HMM AAPM Challenge evaluation methodology.
DVH Area Under Curve (compute_dvh_auc)¶
The integral of the DVH curve, computed via the trapezoidal rule:
$$\text{DVH-AUC} = \int_{d_{\min}}^{d_{\max}} V(d)\, \mathrm{d}d$$
A higher AUC means more of the structure volume receives higher doses. With normalize=True (default) the result is scaled to [0, 1], where 1.0 means 100% of the volume received the maximum dose.
This is a single-distribution metric (unlike compute_area_between_dvh_curves, which computes the difference between two DVH curves).
from dosemetrics.metrics.dvh import compute_dvh_auc
# Normalised AUC for PTV — closer to 1 means better coverage
ptv_auc = compute_dvh_auc(dose, ptv, normalize=True)
# Unnormalised AUC for a serial OAR (Gy·% units)
cord_auc = compute_dvh_auc(dose, spinal_cord, normalize=False)
print(f"PTV DVH-AUC: {ptv_auc:.3f}")
print(f"Cord DVH-AUC: {cord_auc:.1f} Gy·%")
Voxel-Based Accuracy Metrics¶
These metrics compare two dose distributions voxel-by-voxel across the full 3D volume, making them sensitive to localised dose differences that DVH-based metrics can miss.
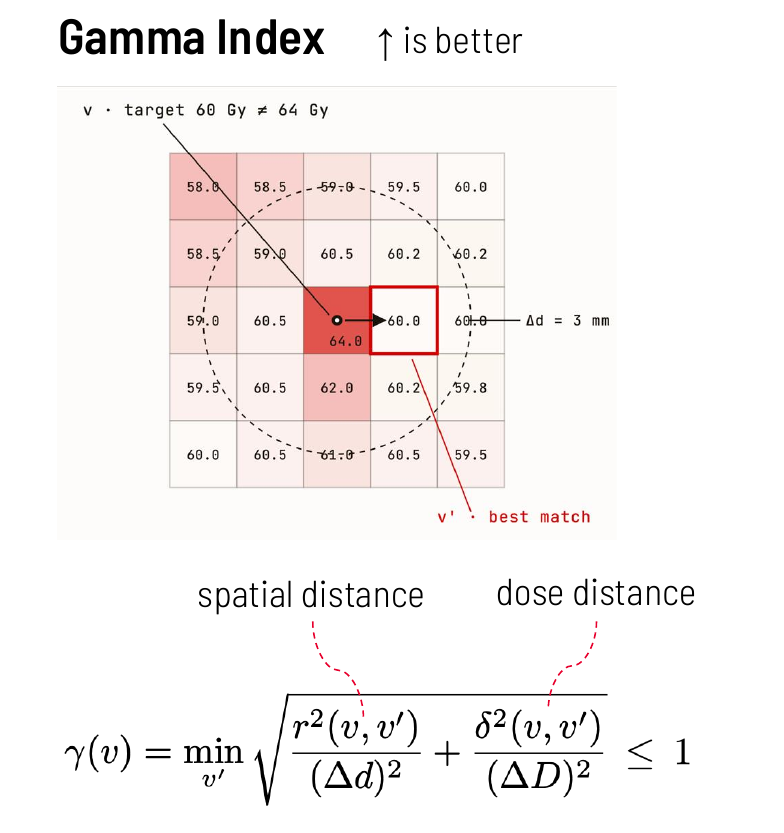 Gamma Index — for each voxel v, the index finds the nearest reference voxel v′ that minimises the combined spatial distance r(v, v′) / Δd and dose distance δ(v, v′) / ΔD. A voxel passes when γ ≤ 1. (Joseph Weibel, MSc Thesis Defense, University of Bern)
Gamma Index — for each voxel v, the index finds the nearest reference voxel v′ that minimises the combined spatial distance r(v, v′) / Δd and dose distance δ(v, v′) / ΔD. A voxel passes when γ ≤ 1. (Joseph Weibel, MSc Thesis Defense, University of Bern)
Normalized MAE (compute_normalized_mae)¶
$$\text{Norm. MAE} = \frac{\text{MAE}(d_{\text{ref}},\, d_{\text{eval}})}{d_{\text{norm}}}$$
A dose comparison MAE scaled by a reference value (e.g., the prescription dose), with optional masking to restrict computation to clinically relevant high-dose voxels.
Setting dose_threshold_gy excludes low-dose background voxels from the average, which avoids diluting the error signal with near-zero differences far from the treatment field.
from dosemetrics.metrics.dose_comparison import compute_normalized_mae
# Normalised by prescription, restricted to high-dose region
n_mae = compute_normalized_mae(
reference_dose,
predicted_dose,
structure=body,
normalization_value=60.0,
dose_threshold_gy=5.0,
)
print(f"Normalized MAE: {n_mae:.4f}") # Dimensionless
Reference: Adapted from ChallengeMAE in the GDP-HMM AAPM Challenge (Gao et al.).
Variance of Laplacian (compute_variance_of_laplacian)¶
$$\text{VoL} = \text{Var}!\left[\nabla^2 d\right]$$
The variance of the Laplacian of the dose distribution, measuring the spatial sharpness of dose gradients. Higher values indicate more complex, high-gradient dose distributions (typical of IMRT/VMAT); lower values indicate smoother, more homogeneous distributions.
The Laplacian highlights rapid spatial changes — steep dose fall-off regions, tongue-and-groove effects, or sharp interface boundaries all contribute to higher VoL.
from dosemetrics.metrics.dose_comparison import compute_variance_of_laplacian
# Global sharpness
vol_global = compute_variance_of_laplacian(dose)
# Sharpness within a structure's volume only
vol_ptv = compute_variance_of_laplacian(dose, structure=ptv)
print(f"Global VoL: {vol_global:.4f}")
print(f"PTV VoL: {vol_ptv:.4f}")
Reference: Adapted from VarianceOfLaplacian in the GDP-HMM AAPM Challenge.
Putting it All Together¶
A typical quality assessment for a single plan:
from dosemetrics.metrics import conformity, homogeneity, dvh, dose_comparison
prescription = 60.0 # Gy
# --- Conformity ---
ci_icru = conformity.compute_conformity_index(dose, ptv, prescription)
ci_rtog = conformity.compute_rtog_conformity_index(dose, ptv, prescription)
ci_pad = conformity.compute_paddick_conformity_index(dose, ptv, prescription)
coverage = conformity.compute_coverage(dose, ptv, prescription)
spillage = conformity.compute_spillage(dose, ptv, prescription)
rx_mae = conformity.compute_prescription_mae(dose, ptv, prescription)
# --- Homogeneity ---
hi = homogeneity.compute_homogeneity_index(dose, ptv)
gi = homogeneity.compute_gradient_index(dose, ptv, prescription)
# --- DVH summary ---
ptv_auc = dvh.compute_dvh_auc(dose, ptv, normalize=True)
stats = dvh.compute_dose_statistics(dose, ptv)
print(f"ICRU CI: {ci_icru:.3f} (ideal 1.0)")
print(f"RTOG CI: {ci_rtog:.3f} (ideal 1.0)")
print(f"Paddick CI: {ci_pad:.3f} (ideal 1.0)")
print(f"Coverage: {coverage * 100:.1f}%")
print(f"Spillage: {spillage * 100:.1f}%")
print(f"Prescription MAE: {rx_mae:.2f} Gy")
print(f"HI (ICRU 83): {hi:.3f} (ideal 0)")
print(f"Gradient Index: {gi:.2f}")
print(f"DVH AUC (PTV): {ptv_auc:.3f}")
print(f"D95: {stats['D95']:.1f} Gy")
Comparing Two Plans¶
from dosemetrics.metrics.dvh import compute_dvh_score
from dosemetrics.metrics.dose_comparison import compute_normalized_mae, compute_variance_of_laplacian
score = dvh.compute_dvh_score(dose_tps, dose_predicted, ptv)
n_mae = dose_comparison.compute_normalized_mae(dose_tps, dose_predicted,
normalization_value=prescription,
dose_threshold_gy=5.0)
sharpness_diff = (
dose_comparison.compute_variance_of_laplacian(dose_predicted)
- dose_comparison.compute_variance_of_laplacian(dose_tps)
)
print(f"DVH Score: {score:.2f} Gy (0 = identical)")
print(f"Normalized MAE: {n_mae:.4f} (0 = identical)")
print(f"Sharpness Δ (VoL): {sharpness_diff:+.4f} (+ = predicted is sharper)")
For DVH visualisation see plot_dvh_comparison and plot_dvh_score_breakdown.
References¶
| Metric | Reference |
|---|---|
| ICRU CI | ICRU Report 62, 1999 |
| van't Riet CN | van't Riet et al., Int J Radiat Oncol Biol Phys, 1997 |
| RTOG CI | Shaw et al., Int J Radiat Oncol Biol Phys, 1993 |
| Paddick CI | Paddick I, J Neurosurg, 2000;93(Suppl 3):219-222 |
| ICRU HI | ICRU Report 83, J ICRU, 2010 |
| Gradient Index | Paddick I & Lippitz B, J Neurosurg, 2006;105(Suppl):194-201 |
| DVH Score | GDP-HMM AAPM Challenge, Gao et al. |
| Normalized MAE | GDP-HMM AAPM Challenge, Gao et al. |
| Variance of Laplacian | GDP-HMM AAPM Challenge, Gao et al. |